



iPhone as the key to a ‘wearable pancreas’ for people living with diabetes
March 28, 2014
by Liza Pliss, Research Consultant, Sachs Insights
"The iPhone is the missing puzzle piece that unlocks the possibility of creating a mobile, stable, closed loop ‘wearable pancreas.’ "
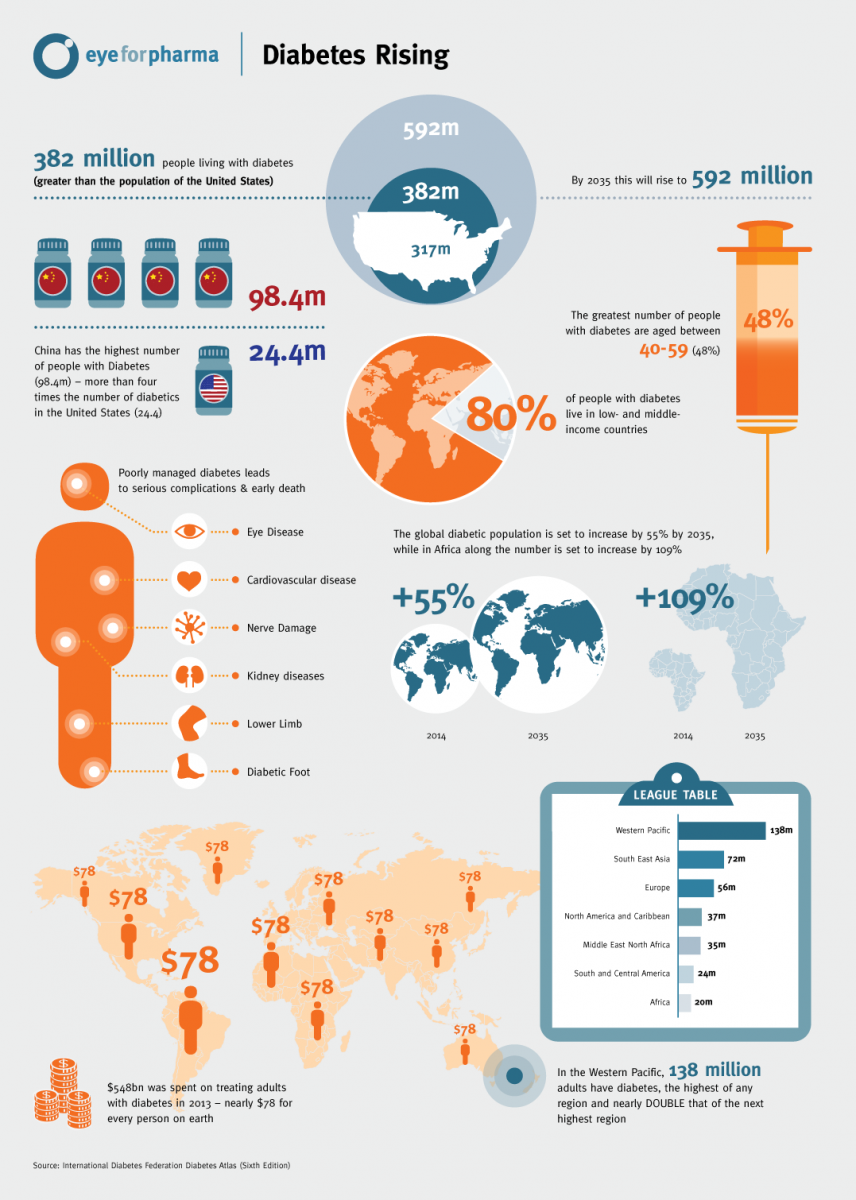
It is 2014 and we are still hearing about people experiencing a diminishing quality of life with diabetes—and many die each year from disease complications. Despite the fact that our knowledge of the disease has expanded to understand contributing causes. Despite the fact that science and medical technology are more precise and better integrated than ever before. We have not yet found a way to prevent Type 1 Diabetes, and we can’t seem to control the climb in prevalence of Type 2 Diabetes.
[tippy title="A diabetes primer (click or roll-over for info)" class="myclass" showheader="true" href="http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002194/#adam_001214.disease... width="450" height="200"]When food is digested, a sugar called glucose enters the bloodstream. Glucose is a source of fuel for the body. In addition, an organ called the pancreas makes insulin. The role of insulin is to move glucose from the bloodstream into muscle, fat, and liver cells, where it can be used as fuel. People with diabetes have high blood sugar because their body cannot move sugar cells to be stored for energy. This is because either their pancreas does not make enough insulin, or their cells do not respond to insulin normally.
Type 1 Diabetes occurs when the pancreas cells required for the body to produce insulin have been destroyed by the body.
Type 2 Diabetes involves a reduced ability for the body to produce or process its own insulin. Both Types of diabetes can be managed with insulin, although Type 2 Diabetes can often be treated with oral medications alone. Insulin or oral medication is supplemented with adherence to diet and exercise.
Source: PubMed
[/tippy]
On the surface, a pancreas transplant may seem like a solution to diabetes. But this involves surgery and high risk that the body will attack the pancreas in a similar manner to the person’s original pancreas. It is rarely considered. Instead, medical innovators are working toward an artificial pancreas. But it’s not really a pancreas at all. It is a linking of several medical devices in a ‘closed loop’ system to calculate and regulate a person’s levels of glucose and insulin—without the person wearing it having to make decisions about what or when to eat, or how much medication to take.
Diabetes management is going okay… sort of…
Those using insulin to manage their diabetes must constantly check their blood glucose levels. They then make decisions about what to eat, how much, and how much insulin to take to make sure their glucose levels do not rise (or fall) too much. The goal is stable levels, but highs and lows seem to happen frequently—even with all the advances in diabetes management. We hear frequently during qualitative market research that many feel their diabetes is not consistently controlled. People describe management of their disease as “exhausting,” “challenging,” and a “non-stop worry.”
We’ve often set out to answer the question of why control seems so elusive. Answers boil down to these factors:
- Lack of education / knowledge about diabetes
- Incorrect / insufficient medication (Type 2 Diabetes)
- Difficulty making and maintaining lifestyle changes
- Challenges with testing blood glucose and administering the right amount of insulin (predominantly Type 1 Diabetes)
The first two factors seem to rest on the shoulders of physicians; the last two are dependent on the patient. For most, living with diabetes is inconvenient at best. Remembering to test blood sugar. Taking the right amount of medication at the right time. Modifying diet and fitness routine. These are challenges along the disease journey. It is here, with human factors playing a large role, where treatment failure—or, at least, lack of success—occurs.
Technology has tried to remove the human brain from the equation as much as possible.
[gallery ids="3452,3450,3451" royalslider="2"]
Smartphones to the rescue
The closed-loop system would find a way for the CGM and the dual chamber pump to “talk” to each other. The CGM would report a glucose level. According to the value from the CGM, insulin and/or glucagon would be administered to the body to maintain the correct levels. Continuously. Without the person having to intervene. Or decide.
Ed Damiano is working on the design of the first commercial bionic pancreas out of Boston University. He explains “if a human could do it, an algorithm could do it, and it could possibly do it better, and certainly more consistently,” referring to the continuous testing, calculating the right dose and self-administering that insulin-users have become accustomed to.
Closing the loop remained elusive until the advent of the smartphone – namely, the iPhone. The iPhone is the missing puzzle piece that unlocks the possibility of creating a mobile, stable, closed loop ‘wearable pancreas.’ The fact that an iPhone allows independent app developers to create their own programs has made the experiment possible. Its impressive computing power, design built for portability and the ability to connect the cellular network at almost any time, made the iPhone the perfect ‘communicator’ between the CGM and the dual chamber pump.
A 2013 trial, published in Diabetes Care reported favorable results, bringing us closer to the possibility of an artificial pancreas. Patients were observed for 42 hours; first with the system operating in open-loop and then, in closed-loop mode. The study that Dr. Kovatchev et al conducted showed 97.7% system functionality from admission to discharge – a remarkably good result, considering the original end point of 80%.[2]
This is exciting for variety of reasons. It removes a great deal of human error and lack of precision out of diabetes management. In fact, a successful closed-loop artificial pancreas will not only ease the burden of therapy for the insulin-dependent but will also improve insulin replacement therapy until glycemic control is practically normal. This will, in turn, decrease incidence of complications (incl. hyper and hypoglycemia; vision loss; neuropathy; kidney failure… The list goes on). Illustration source: http://www.bu.edu/bostonia/summer13/damiano/
Illustration source: http://www.bu.edu/bostonia/summer13/damiano/
The artificial pancreas in the driver’s seat
Reading about the artificial pancreas trial, I was reminded of a podcast I recently listened to on Freakonomics Radio called “The Most Dangerous Machine.”[3] The program focused on automobiles, specifically their safety. Stephen Dubner, the host of the program, articulated: “we are so dependent on our cars, at least for the foreseeable future – but, when driving them, we are our own worst enemy… remember, there are still 1.2 million traffic deaths a year worldwide.” Most accidents are caused by human error or misjudgment.
One possible solution, the driverless car, seems to be a very real possibility in the future. A lot of the necessary technology already exists – GPS systems, on-board computers, sensors and cameras – and has been accepted as the norm. Leaving the decision-making involved in driving to instruments more precise (though less creative) than the human brain seems a no-brainer. In theory, “a computer-operated car will be much safer than a human-operated car. It won’t drive drunk, while putting on mascara, or trying to open the packet of ketchup.”[4]
To me, the parallels between the artificial pancreas and the driverless car are striking. The possibility of having both in the future – exciting.
However, the same reason why this technology is exciting is exactly why it also unnerves some: limiting of human control in the process. Giving up control is uncomfortable. (Rarely is someone called a give-up-control freak.) However, in the case of delivering vital medication or when controlling a 3500 pound moving piece of metal, a failure of technology that is out of the user’s hands is much scarier and carries heavier consequences.
Gaining control by losing control?
So, where does that leave us and what does the possibility of releasing control mean? I oscillate between “this is great” and “this is a really bad idea.” On one hand, this is exactly what the patients we speak to want – a way to push their diabetes to the background and not have to think about it; it is a portal “back to normal.” Having a system that continuously tests blood sugar levels and releases just the right amount of insulin is a little like not having diabetes at all! Most people (and I count myself among them) are happy with the help technology has provided us – the more that is automated and less there is to keep track of, the better.
On the other hand, most people (and I count myself among them as well) are a skeptical bunch. “What if it stops working?” is the most obvious question that comes to mind along with “what if after a long time of not having to test and administer their own medication people actually forget how to take over the automated service?” Actually, that is a question I have of the driverless car: imagine a situation when you’ve been navigating around in a driverless car for 10 years, and one day its brakes stop working suddenly. Now it’s been 10 years since you’ve had to manually drive a car – will you remember how? Is it like riding the proverbial bicycle? And here I am assuming that there are some overriding controls that let the person take over manually – if that doesn’t exist (either in the artificial pancreas or the driverless car), countless more questions arise.
So, the ‘happy techie me’ is excited; the ‘skeptical me’ is dubious. And then there is the ‘researcher me,’ which can’t wait to figure out what will be driving patient and physician decisions. What are the conscious and subconscious considerations that patients will factor in when deciding whether to try out an artificial pancreas? What are some of the emotional factors that will drive action? And then there’s the usability of the device – how easy is it to explain (for physicians) and understand (for patients) the instructions for use? Where do human factors come in, and how high is probability of misuse? And who are these first adapters?
I can’t wait to find out.
[1] Tandem Diabetes Care Announces Partnership with JDRF to Develop Novel Dual-Chamber Infusion Pump. JDRF, January 8, 2013.
[2] Diabetes Care. Ibid.
[3] Dubner, Stephen J. (Host). (2013, December 5). Freakonomics: The Most Dangerous Machine. [Audio podcast]. Retrieved from http://freakonomics.com/2013/12/05/the-most-dangerous-machine-full-transcript/
[4] Ibid.




{kind=link}